Motor Vehicle Collision-Related Injuries in the Elderly, Prevention of
Published 2015
Citation: J Trauma. 79(1):152–158, July 2015
Authors
Crandall, Marie MD, MPH; Streams, Jill MD; Duncan, Thomas DO; Mallat, Ali MD; Greene, Wendy MD; Violano, Pina MSPH, RN-BC, CCRN, PhD; Christmas, A. Britton MD; Barraco, Robert MD; Eastern Association for the Surgery of Trauma Injury Control and Violence Prevention Committee
Author Information
From the Department of Surgery (M.C., J.S.), Northwestern University Feinberg School of Medicine, Chicago, Illinois; Department of Surgery (T.D.), Ventura County Medical Center, Ventura, California; Department of Surgery (A.M.), University of Michigan, Ann Arbor, Michigan; Department of Surgery (W.G.), Howard University Hospital, Washington, District of Columbia; Department of Surgery (P.V.), Yale-New Haven Hospital, New Haven, Connecticut; Department of Surgery (A.B.C)., Carolinas Healthcare Systems, Charlotte, North Carolina; Department of Surgery (R.B.), Lehigh Valley Health Network, Allentown, Pennsylvania.
Submitted: December 8, 2014, Revised: March 12, 2015, Accepted: March 13, 2015.
Address for reprints: Marie Crandall, MD, MPH, Northwestern University Feinberg School of Medicine, 676 N St Clair, Suite 650, Chicago, IL 60611; email:mcrandall@northwestern.edu.
Motor vehicle injury prevention has been termed a “CDC Winnable Battle” because of the significant improvements in motor vehicle–related deaths in the past five decades. The Centers for Disease Control and Prevention [CDC] attributes the dramatic drop in fatalities per million miles traveled to a combination of safer vehicles, safer roadways, and safer driver behaviors.[1] However, despite these advances in car safety, the elderly, defined as individuals 65 years and older, are more likely to die or to be severely injured after motor vehicle collisions (MVCs) than younger people.[2–5]
In 2008, there were more than 30 million licensed drivers 65 years and older in the United States. In that same year, more than 5,500 older Americans were killed, and more than 180,000 were injured in MVCs. As drivers age, fatal crash rates increase in a nonlinear fashion; per mile traveled, they begin to increase at age 75 years and rise steeply after age 80 years.[5] The fatal crash rate increases from approximately 2 per 100 million miles traveled to more than 12 among the oldest drivers.[6] As the elderly population grows in America, we can expect the number of elderly injured by MVCs to increase.
Objectives
The objective of this evidence-based review was to assess the scientific evidence regarding MVC-related injury prevention strategies for elderly (age ≥ 65 years) drivers and pedestrians. Research in the area of motor vehicle safety in the elderly is copious, with well more than 1,000 citations on with a simple search in September 2013. However, few researchers have focused on prevention strategies that use injury as an outcome. The Population (P), Intervention (I), Comparator (C), and Outcome (O) or PICO questions were created using a modified Delphi method by the Eastern Association for the Surgery of Trauma Injury Control and Violence Prevention Committee.
PICO Questions
Population: age of 65 years or greater
Intervention: preventive strategies to reduce injuries from MVCs or auto versus pedestrian incidents.
Comparator: intervention compared with control group.
Outcome: injury from MVCs or auto versus pedestrian incidents,
PICO Question 1. Are car engineering advancements effective at preventing MVC-related injuries among the elderly?
PICO Question 2: Are environmental or behavioral interventions effective at preventing MVC-related injuries among the elderly?
PICO Question 3: Are risk screening strategies effective at preventing MVC-related injuries among the elderly?
Patients and Methods
Inclusion Criteria for This Review
Study Types
Studies included randomized controlled trials, prospective and retrospective observational studies, case-control studies, and meta-analyses. Case reports and reviews containing no original data or analyses were excluded.
Participant Types
We included all studies of motor vehicle–related injury prevention for participants age 65 years or older.
Intervention Types
We included all studies of motor vehicle–related injury prevention methods. Because of the heterogeneity of the interventions, we grouped interventions into the main themes of engineering advancements, environmental and behavioral modifications, as well as risk screening.
Outcome Measure Types
We limited the review to studies in which injury was the outcome, not simply collisions or incidents. Because of the heterogeneity of injury reports, all injuries were felt to be critical to evaluating the literature within the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework.
Review Methods
Search Strategy
References were identified by research librarians using the Cochrane Library, and the MEDLINE database in the National Library of Medicine and the National Institutes of Health was searched using Entrez (www.pubmed.gov) in November 2012. The search was designed to identify all English language citations regarding motor vehicle–related injury prevention in the elderly. In addition to the electronic search, we manually searched the bibliographies of recent reviews and articles. Finally, we performed focus search updates in November 2013 and November 2014, during the review and manuscript preparation stages. Figure 1 contains the MeSH terms used for the initial search.
Study Selection
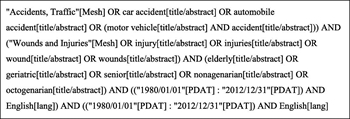
Figure 1: MeSH search terms.
After completing a comprehensive literature search, three independent reviewers screened the titles and abstracts, excluding reviews, case reports, articles in which injury was not the outcome measure, and unrelated articles. The resulting studies were used for the review. The study selection process is highlighted in the PRISMA flow diagram for Figure 2.
Data Extraction and Management
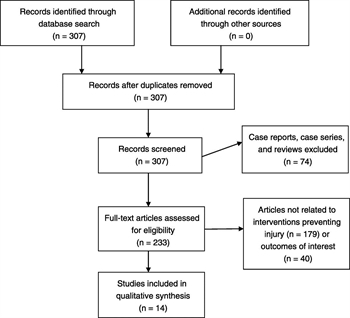
Figure 2: PRISMA flow diagram.
All studies used for the review were entered into a Microsoft Excel spreadsheet containing information on authors, article title, study methodology, as well as intervention and outcome measures. A master copy was provided to all reviewers.
Methodological Quality Assessment
We used the validated GRADE methodology for this study.[7][8] The GRADE methodology entails the creation of a predetermined PICO question or set of PICO questions that the literature must answer. Each designated reviewer independently evaluated the data in aggregate with respect to the quality of the evidence to adequately answer each PICO question and quantified the strength of any recommendations. Reviewers are asked to determine effect size, risk of bias, inconsistency, indirectness, precision, and publication bias.
Recommendations are based on the overall quality of the evidence. GRADE methodology suggests the phrases, “we strongly recommend” for strong evidence and “we suggest” or “we conditionally recommend” for weaker evidence.
Results
We found 14 articles regarding MVC-related injury prevention among the elderly addressing our three main areas of interest: car engineering, environmental and behavioral interventions, as well as risk screening strategies. Each evidence profile was evaluated separately as it related to our predetermined PICO question.
PICO Question 1: Car Engineering Advancements
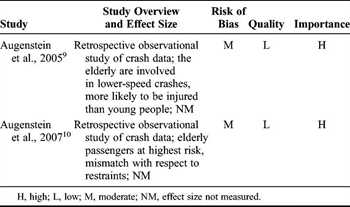
TABLE 1: Strength of Evidence for Car Engineering Advancements in the Prevention of MVC-Related Injuries in the Elderly
Automobile safety features have evolved and advanced during the previous decades with a goal of injury reduction in the event of a collision. However, the literature regarding how these safety features, such as seat belts and airbags, perform with elderly vehicle occupants is limited. In 2005, Augenstein et al.[9] published the results of a retrospective investigation of the National Automotive Sampling System–Crashworthiness Data System database from 1997 to 2003. The data concluded that individuals 65 years or older are more likely to be involved in lower-speed collisions; in addition, they are more likely to have a Maximum Abbreviated Injury Scale (MAIS) score of 3 or higher injuries from these lower-severity crashes compared with younger counterparts. Not surprisingly, the risk of MAIS score 3+ injury increases with the speed of the crash, but the probability of injury is higher in elderly vehicle occupants, indicating a lower injury tolerance in the elderly. The authors suggest the need for chest protection measures such as lower force airbags and more adaptable seat belt restraint systems. A related investigation of the same database examined frontal crashes and compared relative risk of injury for drivers and front seat passengers stratified by sex and age.[10] Elderly occupants were more at risk for injury or death than elderly drivers; when both the vehicle driver and the front seat occupant were elderly, the passenger had a 42% higher risk of fatality. The authors called for more benign passenger safety restraint systems to reduce injuries, particularly injuries to the chest (Table 1).
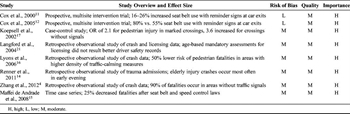
TABLE 2: Strength of Evidence for Environmental and Behavioral Interventions to Prevent MVC-Related Injuries in the Elderly
PICO Question 2: Environmental and Behavioral Interventions
Strategies of injury prevention in the elderly MVC patient include those of environmental and behavioral interventions. For example, the simple intervention of posting a seat belt use reminder sign at an intersection outside five senior communities increased the percentage of drivers wearing seat belts from 72% to 94%.[11] At 4-year follow-up, this intervention had a durable but diminished effect, with approximately 80% of vehicle occupants using seat belts.[12] This is far superior to the 55% rate of seat belt use at case-matched control centers without seat belt reminder signage. Other behavioral interventions may be self-imposed by elderly drivers such as avoiding driving in urban areas, during heavy traffic times, or at night.[13] However, the elderly population has been demonstrated to have a higher rate of collisions resulting in injuries during the early evening hours compared with younger drivers as reported by Renner et al.[14] This may reflect a sundowning effect of diminished motor and sensory function for elderly drivers in the evening hours.
Environmental interventions to reduce MVCs generally focus on accident prevention among all ages, but with the knowledge that the elderly have the highest mortality rate of any age group when involved in an MVC.[15] A descriptive series of MVC fatalities in a Brazilian city reports minor reductions in mortality for individuals of all ages with the institution of mandatory seat belt use, targeted speed radar use, and improved prehospital care of MVC patients. A 28.4% reduction in MVC mortality was seen after the adoption of a traffic safety code. Lyons et al.[16] demonstrated that traffic-calming measures can be implemented to combat pedestrian injuries and decrease fatalities among all age groups. A group from China performed an analysis of an accident database and reported that the elderly were involved in only 11.7% of MVCs but accounted for 23.4% of mortalities.[4]Pedestrians accounted for the majority of casualties, and approximately 90% of accidents occurred on roadways without traffic signals. These findings were confirmed by a report from Koepsell et al.[17] in 2002. They performed a case-control study examining elderly pedestrian MVC accidents at crosswalks and reported an overall increased odds ratio (OR) of 2.1 for a collision at a marked crosswalk, as opposed to a crosswalk with a traffic signal or stop sign. In particular, there was an OR of 3.6 for pedestrian MVC collision at a marked crossing on roads without traffic signals (Table 2).
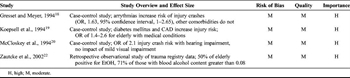
TABLE 3: Strength of Evidence for Risk Screening Strategies in the Prevention of MVC-Related Injuries in the Elderly
PICO Question 3: Risk Screening Strategies
Risk screening strategies are another area of elderly MVC injury prevention, which seeks to identify characteristics of elderly drivers at higher risk for being involved in MVCs. Several studies have investigated comorbid medical conditions in the elderly that may place them at increased risk of injury crashes. Gresset and Meyer[18] performed a case-control study of the medical history of 1,400 drivers in their 70th year involved in crashes compared with 2,636 age-matched control drivers. They report that arrhythmias were the only comorbid condition that significantly increased the risk of MVC. A similar study by Koepsell et al.[19] revealed an increased OR for MVC in elderly drivers with diabetes and coronary artery disease (CAD) (OR, 1.4–2.6). In particular, elderly diabetic drivers treated with insulin or oral hypoglycemic or those with long-standing diabetes were at increased risk of crashes.
Other studies have focused on whether age-related sensory deficits contribute to increased risk for elderly drivers. McCloskey et al.[20] found that diminished visual acuity did not increase the risk of MVC injury in the elderly; however, they did report that elderly drivers using a hearing aid while driving had an increased OR of 2.1 for injury in a crash. Based on these findings, many countries have instituted mandatory medical screenings as a condition for licensure in the elderly. Yet, medical screenings alone may not prove a significant risk reduction strategy.[21] Since driving is a complex task that involves physical motor skills, multiple sensory inputs, cognitive processing, and attention, the mere presence of a comorbid medical condition in elderly drivers may not be a useful determinant of driver safety.
It has been well established that alcohol or drug intoxication significantly increases the risk of being involved in an MVC. The elderly population may be even more sensitive to the effects of drugs and alcohol than their younger counterparts because of age-related derangements in metabolism, comorbid medical conditions, and medication interactions. Significantly, a retrospective analysis of Illinois trauma patients reported that while only 5% of elderly trauma patients were tested for alcohol or drug use, 50% of those tested were positive.[22] In addition, 71% of elderly trauma patients with a positive alcohol screen result were found to be legally intoxicated with a blood alcohol content greater than 0.08 mg/dL. This indicates a need for continued alcohol abuse screening in elderly drivers (Table 3).
Discussion
MVC-related injuries are a significant problem among the elderly, but injury prevention research is lagging. After a rigorous literature review, we were only able to find 14 articles that met our inclusion criteria, studies that directly assessed the risk of injury after MVCs, and only 2 of these were direct intervention trials.
Recommendations
PICO Question 1: Are car engineering advancements effective at preventing MVC-related injuries among the elderly?
Recommendation: We suggest that ongoing engineering advancements in car safety restraint systems begin to take into account passenger-specific factors such as age, weight, and height.
As the US population proportionally ages, the number of elderly drivers can be expected to increase. The literature has demonstrated that elderly drivers are at significant risk of injury when involved in an MVC as a driver, passenger, or pedestrian. The current safety restraint standards for vehicles in the United States do not take into account the vulnerability to injury of elderly vehicle occupants. In low-speed collisions, the very restraint systems designed to prevent injury may be contributing to chest/torso injuries in the elderly. An ideal solution would entail the development and implementation of sex-, height-, and weight-sensitive restraints to protect elderly occupants.
PICO Question 2: Are environmental or behavioral interventions effective at preventing MVC-related injuries among the elderly?
To answer this question, we found two subsets of data, one subset addressing reminder signs for seat belt use (2a) and the other subset addressing traffic-calming measures (2b).
PICO 2a: We recommend that seat belt reminder signs are placed at exit points in areas with significant numbers of senior drivers, such as senior centers or assisted living facilities.
Elderly drivers are more likely to be injured by similar velocity crashes. Based on prospective interventional data collected in multicentered trials, seniors successfully responded to seat belt reminders, and the effects were sustained with time.
PICO 2b: We suggest that pedestrian crosswalks be marked with stop signs or traffic lights and that traffic-calming measures be considered in areas of high pedestrian density.
The elderly are at high risk of injury as pedestrians struck by cars. However, it seems that unmarked crosswalks, that is, ones without stop signs or traffic lights, are associated with increased injury risk. Pedestrians may consider a crosswalk to be safe simply because it is a crosswalk, without considering driver cues or behaviors. In addition, lowering speeds and adding speed bumps or traffic circles in higher-trafficked areas was associated with fewer fatal pedestrian crashes. These should be considered but may also have important implications for businesses and residents.
PICO Question 3: Are risk screening strategies effective at preventing MVC-related injuries among the elderly?
PICO 3: We suggest that elderly should be screened for alcohol abuse, frailty, significant diabetes, hearing impairments, severe visual impairments, and CAD if they are continuing to drive because these conditions are known to increase the risk of MVC-related injuries.
Behavioral interventions to prevent MVC-related injury have been shown to be effective for elderly drivers. These types of programs aim to change elderly driver behaviors to enhance their safety and reduce injury. Seat belt awareness programs can be successful in changing the habits of a generation that did not have mandatory seat belt laws. However, the research on other behavioral interventions is lacking. There is a need for additional direct intervention investigations. Risk reduction strategies strive to identify key risk factors that place elderly drivers at higher risk for MVCs and injury. Several medical conditions such as arrhythmias, CAD, diabetes, and hearing impairment have been implicated. Universal screening for alcohol and drug abuse or use causing driving impairment, irrespective of age, should be a goal. Finally, frailty has been increasingly found to be associated with injury outcomes;[23][24] frailty assessment may be a useful tool to help identify at-risk aging drivers, and its predictive ability should be prospectively studied.
It must be noted that the elderly driver population is heterogeneous; thus, any generalized limitation on driving privileges based on medical conditions is not indicated; individual patients should be screened for significant impairments that might affect their ability to drive safely.
Conclusion
In summary, the paucity of controlled studies in the area of motor vehicle–related injury prevention among the elderly demonstrates a significant information gap, and this committee recommends further research to strengthen future evidence-based guidelines. Of note, our PICO questions deliberately focused on prevention programs that had been tested; other strategies, such as graduated driving laws for seniors, have been posited but not rigorously examined. Future topical updates will require reevaluation of these and other potentially useful injury prevention strategies.
Authorship
M.C. was responsible for the conceptualization, evidence grading, and manuscript preparation. A.M., P.V., R.B., A.B.C., and T.D. were responsible for the evidence grading and manuscript editing. J.S. was responsible for the manuscript preparation.
Disclosure
The authors declare no conflicts of interest.
References
- Centers for Disease Control and Prevention. Ten Significant Public Health Achievements—United States, 2001–2010: Motor Vehicle Safety. 2013. Available at:http://www.cdc.gov/Motorvehiclesafety/mmwr_achievements.html. Accessed March 2013.
- Hui T, Avital I, Soukiasian H, Margulies DR, Shabot MM. Intensive care unit outcome of vehicle-related injury in elderly trauma patients. Am Surg. 2002; 68 (12): 1111–1114.
- Mosenthal AC, Livingston DH, Lavery RF, Knudson MM, Lee S, Morabito D, Manley GT, Nathens A, Jurkovich G, Hoyt DB, et al. The effect of age on functional outcome in mild traumatic brain injury: 6-month report of a prospective multicenter trial. J Trauma. 2004; 56 (5): 1042–1048.
- Zhang L, Zhou JH, Qiu J, Zhang XZ, Yuan DF, Gao ZM, Dai W. Comparative analysis of characteristics and risk factors of traffic injury in aged people from urban and rural areas in Chongqing. Chin J Traumatol. 2012; 15 (1): 27–31.
- Centers for Disease Control and Prevention. CDC Fact Sheet–Older Adult Drivers: Get the Facts. Atlanta, GA. 2013. Available at:http://www.cdc.gov/Motorvehiclesafety/Older_Adult_Drivers/adult-drivers_factsheet.html Accessed March 2013.
- Massie D, Campbell K. Analysis of accident rates by age, gender, and the time of day based on the 1990 nationwide personal transportation survey. Ann Arbor, MI: University of Michigan, Institute TR; 1993. Contract No.: UMTRI-93-7.
- Jaeschke R, Guyatt GH, Dellinger P, Schünemann H, Levy MM, Kunz R, Norris S, Bion J, GRADE Working Group. Use of GRADE grid to reach decisions on clinical practice guidelines when consensus is elusive. Br Med J. 2008; 337: a744.
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schünemann HJ, GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Br Med J. 2008; 336 (7650): 924–926.
- Augenstein J, Digges K, Bahouth G, Dalmotas D, Perdeck E, Stratton J. Investigation of the performance of safety systems for protection of the elderly. Annu Proc Assoc Adv Automot Med. 2005; 49: 361–369.
- Augenstein J, Perdeck E, Digges K, Bahouth G. Age appropriate restraints for the right front passenger. Annu Proc Assoc Adv Automot Med. 2007; 51: 381–394.
- Cox BS, Cox AB, Cox DJ. Motivating signage prompts safety belt use among drivers exiting senior communities. J Appl Behav Anal. 2000; 33 (4): 635–638.
- Cox CD, Cox BS, Cox DJ. Long-term benefits of prompts to use safety belts among drivers exiting senior communities. J Appl Behav Anal. 2005; 38 (4): 533–536.
- Naumann RB, Dellinger AM, Kresnow MJ. Driving self-restriction in high-risk conditions: how do older drivers compare to others? J Safety Res. 2011; 42 (1): 67–71.
- Renner CH, Heldt KA, Swegle JR. Diurnal variation and injury due to motor vehicle crashes in older trauma patients. Traffic Inj Prev. 2011; 12 (6): 593–598.
- Maffei de Andrade S, Soares DA, Matsuo T, Barrancos Liberatti CL, Hiromi Iwakura ML. Road injury-related mortality in a medium-sized Brazilian city after some preventive interventions. Traffic Inj Prev. 2008; 9 (5): 450–455.
- Lyons RA, Jones SJ, Newcombe RG, Palmer SR. The influence of local politicians on pedestrian safety. Inj Prev. 2006; 12 (5): 312–315.
- Koepsell T, McCloskey L, Wolf M, Moudon AV, Buchner D, Kraus J, Patterson M. Crosswalk markings and the risk of pedestrian-motor vehicle collisions in older pedestrians. JAMA. 2002; 288 (17): 2136–2143.
- Gresset J, Meyer F. Risk of automobile accidents among elderly drivers with impairments or chronic diseases. Can J Public Health. 1994; 85 (4): 282–285.
- Koepsell TD, Wolf ME, McCloskey L, Buchner DM, Louie D, Wagner EH, Thompson RS. Medical conditions and motor vehicle collision injuries in older adults. J Am Geriatr Soc. 1994; 42 (7): 695–700.
- McCloskey LW, Koepsell TD, Wolf ME, Buchner DM. Motor vehicle collision injuries and sensory impairments of older drivers. Age Ageing. 1994; 23 (4): 267–2673.
- Langford J, Fitzharris M, Newstead S, Koppel S. Some consequences of different older driver licensing procedures in Australia. Accid Anal Prev. 2004; 36 (6): 993–1001.
- Zautcke JL, Coker SB Jr, Morris RW, Stein-Spencer L. Geriatric trauma in the State of Illinois: substance use and injury patterns. Am J Emerg Med. 2002; 20 (1): 14–17.
- Joseph B, Pandit V, Zangbar B, Kulvatunyou N, Tang A, O’Keeffe T, Green DJ, Vercruysse G, Fain MJ, Friese RS, et al. Validating trauma-specific frailty index for geriatric trauma patients: a prospective analysis. J Am Coll Surg. 2014; 219 (1): 10–17.e1.
- Joseph B, Pandit V, Zangbar B, Kulvatunyou N, Hashmi A, Green DJ, O’Keeffe T, Tang A, Vercruysse G, Fain MJ, et al. Superiority of frailty over age in predicting outcomes among geriatric trauma patients: a prospective analysis. JAMA Surg. 2014; 149 (8): 766–772.