Contact Sports-related Concussion in Amateur Athletes, Primary Prevention of (UPDATE IN PROGRESS)
Published 2018
Citation: Trauma Surg Acute Care Open 2018;3:e000153. doi:10.1136/tsaco-2017-000153
Authors
Toby M Enniss, Khaled Basiouny, Brian Brewer, Nikolay Bugaev, Julius Cheng, Omar K Danner, Thomas Duncan, Shannon Foster, Gregory Hawryluk, Hee Soo Jung, Felix Lui, Rishi Rattan, Pina Violano, Marie Crandall
Author Information
From the Department of Surgery, University of Utah School of Medicine (T.E.), Salt Lake City, Utah; Department of Trauma Surgery, George Washington University School of Medicine and Health Sciences (K.B.), Washington, Columbia; Department of Surgery, Indiana University School of Medicine (B.B.), Indianapolis, Indiana; Department of Surgery, Tufts University School of Medicine (N.B.), Boston, Massachusetts; Department of Surgery, University of Rochester Medical Center (J.C.), Rochester, New York; Department of Surgery, Morehouse School of Medicine (O.D), Atlanta, Georgia; Department of Trauma Services, Ventura County Medical Center (T.D.), Ventura, California; Department of Trauma and Surgical Critical Care, University of Pennsylvania Reading Hospital (S.F.), West Reading, Pennsylvania; Department of Neurosurgery, University of Utah School of Medicine (G.H.), Salt Lake City, Utah; Department of Surgery, University of Wisconsin School of Medicine and Public Health (H.S.J.), Madison, Wisconsin; Department of Surgery, Yale School of Medicine (F.L.), New Haven, Connecticut; Department of Surgery, University of Miami Miller School of Medicine (R.R.), Miami, Florida; Injury Prevention, Community Outreach and Research, Yale-New Haven Hospital (P.V.), New Haven, Connecticut; Department of Surgery, University of Florida College of Medicine-Jacksonville (M.C.), Jacksonville, Florida
Received: December 14, 2017, Accepted: May 11, 2018, First published: June 20, 2018
Correspondence to: Dr Toby M Enniss, Department of Surgery, University of Utah School of Medicine, Salt Lake City, UT 84132, USA; [email protected]
Abstract
Background Awareness of the magnitude of contact sports-related concussions has risen exponentially in recent years. Our objective is to conduct a prospectively registered systematic review of the scientific evidence regarding interventions to prevent contact sports-related concussions.
Methods Using the Grading of Recommendations Assessment, Development, and Evaluation methodology, we performed a systematic review of the literature to answer seven population, intervention, comparator, and outcomes (PICO) questions regarding concussion education, head protective equipment, rules prohibiting high-risk activity and neck strengthening exercise for prevention of contact sports-related concussion in pediatric and adult amateur athletes. A query of MEDLINE, PubMed, Scopus, Cumulative Index of Nursing and Allied Health Literature, and Embase was performed. Letters to the editor, case reports, book chapters, and review articles were excluded, and all articles reviewed were written in English.
Results Thirty-one studies met the inclusion criteria and were applicable to our PICO questions. Conditional recommendations are made supporting preventive interventions concussion education and rules prohibiting high-risk activity for both pediatric and adult amateur athletes and neck strengthening exercise in adult amateur athletes. Strong recommendations are supported for head protective equipment in both pediatric and adult amateur athletes. Strong recommendations regarding newer football helmet technology in adult amateur athletes and rules governing the implementation of body-checking in youth ice hockey are supported.
Conclusion Despite increasing scientific attention to sports-related concussion, studies evaluating preventive interventions remain relatively sparse. This systematic review serves as a call to focus research on primary prevention strategies for sports-related concussion.
Level of evidence IV.
PROSPERO registration number #42016043019.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
http://dx.doi.org/10.1136/tsaco-2017-000153
Introduction
Concussion in sports has come to the forefront of both scientific and public awareness, manifested by the exponential increase in research from less than 100 articles published annually during the 1980s to over 900 during 2016.[1] Concomitantly, numerous evidence-based guidelines have been generated,[2–7] focusing on topics such as sideline assessment, diagnostic evaluation, management, and prevention of secondary concussion.
A major tenet of modern trauma care is primary prevention of injury. However, as it relates to sports-related concussion, interventions promoted in existing guidelines have not been critically examined for efficacy. A recent, comprehensive systematic review and meta-analysis published in 2017 by Emery et al [8] added significantly to the body of knowledge on this topic. Our goals were to complement this work using the validated Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology to create specific a priori questions, limit our literature review to publications which meet predefined criteria, and develop recommendations for practitioners.
Our objective was to systematically evaluate the scientific evidence regarding preventive interventions promoted in existing guidelines, such as protective headgear, concussion education, neck mass exercise, and rule modification for pediatric and adult amateur athletes. We focused on two distinct populations in whom the issue of concussion prevention is relevant: pediatric athletes (age 14 or younger) and adult amateur athletes (non-professionals aged 15 years and older), maintaining the results broadly applicable to the general population. Our single, critical outcome was the incidence of contact sports-related concussion.
PICO questions
PICO 1: In pediatric athletes, should players, parents, and coaches receive concussion education (vs no such education) to reduce the incidence of sports-related concussion?
PICO 2: In adult amateur athletes, should players and coaches receive concussion education (vs no such education) to reduce the incidence of sports-related concussion?
PICO 3: In pediatric athletes, should a particular type of head protective equipment be worn to reduce the incidence of sports-related concussion?
PICO 4: In adult amateur athletes, should a particular type of head protective equipment be worn to reduce the incidence of sports-related concussion?
PICO 5: For pediatric athletes, should rule modifications governing high-risk activity (vs no such activity restriction) be instituted to reduce the incidence of sports-related concussion?
PICO 6: For adult amateur athletes, should rule modifications governing high-risk activity (vs no such activity restriction) be instituted to reduce the incidence of sports-related concussion?
PICO 7: In adult amateur athletes, should exercises to increase neck mass be performed (vs no such directed exercise) to reduce the incidence of sports-related concussion?
Methods
A workgroup from the Injury Control and Violence Prevention Committee of the Eastern Association for the Surgery of Trauma (EAST) conducted a systematic review of the evidence addressing prevention of contact sports-related concussions.
Our seven questions were formulated a priori in the PICO format (patient population, intervention, comparator, and outcome) per the GRADE methodology[9][10] over three rounds using a modified Delphi method. This systematic review was prospectively registered with PROSPERO (#42016043019).
Identification of references
The literature search was performed by a university-affiliated research librarian. A preliminary query revealed no pertinent articles prior to 1985. Therefore, a comprehensive search of the literature from January 1, 1985 to November 30, 2017 was conducted using MEDLINE, PubMed, Scopus, Cumulative Index of Nursing and Allied Health Literature, and Embase (online supplementary appendix A). The references of all publications directly addressing prevention of sports-related concussion were reviewed to identify additional potentially pertinent articles.
Inclusion and exclusion criteria for systematic review
Studies were included if they reported original data, were published in English, and evaluated the relationship between the designated interventions and contact sports-related concussion. Articles containing no original data, expert opinion only, or evaluating non-contact-sports-related concussions were excluded. No unpublished data were reviewed. In instances of disagreement on inclusion, thorough discussion of each viewpoint occurred and the final consensus was followed. There were no studies for which a consensus was not reached.
Data extraction
All studies were reviewed by each member of a subgroup consisting of five to six members dedicated to a specific PICO question. Extracted data included study methodology, intervention, and outcome measures. Discrepancies in extracted data were resolved by the primary author.
Results

FIGURE 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram. GRADE, Grading of Recommendations Assessment, Development, and Evaluation; PICO, population,intervention, comparator, and outcomes.
The search returned 1053 references. Titles were screened for relevance, identifying 37 potentially pertinent articles. The references of these articles were reviewed, identifying 106 additional potentially pertinent articles. Abstracts for these 143 articles were reviewed by the working group, narrowing articles for full-text review to 54. Subgroups then undertook a detailed review of all articles relevant to individual PICO questions, identifying 31 articles for inclusion (Figure 1). These include three randomized control trials, all of which contain significant methodologic flaws. The remaining 28 studies were uncontrolled retrospective cohort or prospective observational studies. The number of pertinent studies per PICO question ranged from 1 study evaluating concussion education in adult amateur athletes to 14 studies evaluating various aspects of head protective equipment in adult amateur athletes.
Quality assessment
Each reviewer independently evaluated article quality with regard to study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, size of effect, dose response, and minimization of confounding variables as per the GRADE methodology.[11]
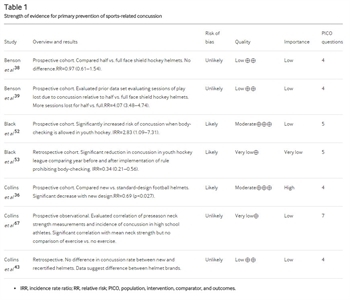
TABLE 1. Strength of evidence for primary prevention of sports-related concussion
Discussion
Formulation of recommendations
In formulating recommendations, the GRADE methodology identifies four factors that contribute to the strength of a recommendation: quality of the evidence, balance between desirable and undesirable effects of intervention, values and preferences of the population, and cost of intervention.[12] A strong recommendation is made if, in considering these four factors, most people to whom the recommendation would apply would want the recommended intervention and only a small proportion would not, whereas a conditional recommendation is given if many people would want the recommended intervention but many would not.
Concussion education in pediatric athletes (PICO 1)
Concussion education has been suggested as a primary preventive intervention[13][14] and several programs have been developed, such as the Centers for Disease Control and Prevention’s (CDC) ‘HEADS UP’ program.[15][16] Presently, all 50 states and the District of Columbia have some form of youth sports concussion law, many mandating concussion education.
Our review identified four studies evaluating education programs in pediatric athletics. Cook et al [17] demonstrated a significant reduction in the high-risk activities of cross-checking and checking from behind among hockey players after one mid-season showing of ‘Smart Hockey’ by the ThinkFirst Foundation of Canada. Covassin et al [18] demonstrated improved attitude toward and ability to identify concussion among youth coaches after use of the CDC’s ‘HEADS UP’ program but did not evaluate impact on concussion incidence. Cusimano et al [19] found that hockey players who viewed the educational video ‘Smart Hockey’ demonstrated an increase in concussion-specific knowledge but found no significant change in behavior or aggression. Kerr et al[20] demonstrated a significant reduction in risk of concussion during practice but not in overall rate of concussion with implementation of the USA Football program ‘Heads Up Football’ in youth football.
The increased awareness and knowledge among athletes, parents, and coaches and the possible decrease in high-risk activities are desirable effects of concussion education programs. Undesirable effects of implementing a concussion education program would be minimal and would include time taken away from practice and inattention among athletes for an activity not involving participation in the sport. Considering these factors, the consensus is that many involved in pediatric athletics would choose a concussion education program versus no formal education as a strategy for the primary prevention of concussion, although many may not.
Recommendation: Conditional recommendation for concussion education as a primary preventive intervention against concussion in pediatric athletes.
Concussion education in adult amateur athletes (PICO 2)
One study was found which considered athletes 15 years of age or older. Kerr et al [21] demonstrated a significant reduction in risk of concussion using the ‘Heads Up’ program in high school football.
The additional factors discussed for pediatric athletes would also apply to adult amateur athletes. Our consensus is that many adult amateur athletes would choose a concussion education program versus no formal education as an intervention for the primary prevention of concussion, although many may not.
Recommendation: Conditional recommendation for concussion education as a primary preventive intervention against concussion in adult amateur athletes.
Head protective equipment in pediatric athletes (PICO 3)
For primary concussion prevention, the most intuitive strategy would be protective headgear. Helmets are effective in decreasing the incidence of severe head trauma in bicyclists[22][23] and recreational skiers and snowboarders.[24–26] There also exists evidence suggesting a decreased risk of concussion among recreational bicyclists with the use of protective helmets.[27]
Our review found three studies evaluating padded headgear use in pediatric contact sports. All three included athletes over 14 years of age in their analysis.
McIntosh and McCrory[28] compared the use of padded headgear versus none in rugby and found no difference in concussion incidence, possibly influenced by a high rate of non-compliance with randomization. McIntosh et al [29] randomized rugby players to wear standard thickness headgear (10 mm thick padding), modified headgear (16 mm thick padding), or no headgear, again with substantial non-compliance among subjects. Analysis, per protocol and by intention-to-treat, demonstrated no difference in concussion incidence.
Delaney et al [30] surveyed soccer players to evaluate the correlation of padded headgear use with self-reported symptoms of concussion, arguably an indirect and imprecise measure, and found a relative risk (RR) of 2.65 in players not wearing headgear (p<0.0001).
The desirable effects of definite reduction in severe head injury in athletic and recreational activities[22–26] and literature suggesting a similar effect for concussion compare very favorably with the undesirable effects of increased cost of equipment and a possible negative impact on athletic performance. The acceptance of head protective equipment in a wide variety of activities reflects the value placed on injury prevention by the general population. The balance of these factors would lead to the conclusion that most pediatric athletes and their parents would want to use head protective equipment as primary prevention of concussion, and only a small proportion would not.
Recommendation: Strong recommendation for head protective equipment as a primary preventive intervention against concussion in pediatric athletes.
Head protective equipment in adult amateur athletes (PICO 4)
Protective headgear reduces the risk of severe head injuries in adult athletes[22][23] as well as in recreational winter sports.[24][26][31] A trend toward decrease in mild traumatic brain injury in rugby players wearing headgear has been suggested.[32] Our review yielded 14 studies evaluating head protective equipment and concussion in adult amateur athletes engaging in contact sports.
The three studies discussed in PICO 3 included athletes older than 14, but did not separate out data based on age.[28–30]
Zemper[33] in 1989 evaluated concussion incidence relative to the brand of helmet in college football and identified no significant difference. A later study by Zemper[34] in 1994 compared concussion rates for 10 models of collegiate football helmets over a longer time frame. Two models were shown to have a higher than expected rate of concussion and one model to have a lower than expected rate. The outlier models were not identified and there was no discussion of what might account for the difference.
Historically, impacts in laboratory helmet testing were not allowed to be delivered distal to the basic plane of the head (the plane defined by the external auditory meatus and inferior orbital notch). In 2003, it was demonstrated that 36% of live impacts resulting in concussion occurred distal to this plane.[35] This led to change in helmet design in which the exterior shell was extended distally over the zygoma and mandible with increased padding beneath the shell. Collins et al [36] found a significant decrease in concussion incidence with this newer helmet technology compared with the older design, 5.3% versus 7.6% (p<0.027), representing a 31% decrease in risk (RR=0.69).Risk reduction was also observed in the subgroup with no prior concussion, 3.7% versus 6.2% (p<0.009) with a relative risk of 0.59. Rowson et al [37] similarly demonstrated a risk reduction of 0.46 (0.28–0.76) when comparing the newer with older design in collegiate football.
Benson et al [38] in 1999 showed no difference in concussion risk but identified increased concussion severity, defined as playing time lost due to concussion, associated with half versus full face shields in collegiate hockey. Benson et al [39] later in 2002 demonstrated no difference in incidence of concussion, but increased playing time missed for concussions associated with half face shields. This remained significant when comparing game versus practice, forward versus defense positions, new versus recurrent concussion, and rookie versus veteran experience level. The authors concluded that the severity of concussion is significantly greater with half versus full face shields.
Stuart et al [40] evaluated the impact of no versus half versus full face shields in adult amateur hockey players, finding incidences of concussion of 12.2, 8.2 and 2.9 per 100 player hours, respectively (p=0.11).
Marshall et al [41] investigated injury prevention effectiveness of padded headgear and mouth guards in rugby players and demonstrated no protective effect of either against concussion.
McGuine et al [42] found no difference in concussion incidence between helmet brands in high school football. Collins e t al [43]demonstrated a non-significant difference between helmet brands and no significant difference in the rate of concussion between new and recertified football helmets.In evaluating helmet liners, Greenhill et al [44] demonstrated increased rate and severity of concussion for air bladder compared with foam or gel liners in high school football.
Consideration of factors similar to the discussion for pediatric athletes together with the more definitive demonstration of the benefit of head protective equipment in adults led us to conclude that most adult amateur athletes would want to use head protective equipment as a primary preventive intervention against concussion, and only a small proportion would not.
Recommendation: Strong recommendation for head protective equipment as a primary preventive strategy against concussion in adult amateur athletes. The evidence also supports a specific strong recommendation for newer football helmet technology as an effective strategy for the primary prevention of concussion in adult amateur football players.
High-risk activity regulation in pediatric athletes (PICO 5)
The most common cause of concussion in sports is player-to-player contact.[45] Rule changes have been implemented to prohibit certain high-risk forms of contact, such as helmet-to-helmet tackling in football, allowable player-to-player contact in soccer, and specific forms of checking in ice hockey. The Consensus Statement on Concussion in Sport from the Fourth International Conference on Concussion in Sport states that ‘rule enforcement may be a critical aspect of modifying injury risk’.[7] Our search of the literature revealed 10 articles addressing rule changes and incidence of concussion in pediatric athletes.
In the 1990s, several instances of rule changes occurred lowering the age at which body-checking was permitted. These changes were partially based on the argument that learning proper technique to deliver and receive contact would lead to reduced injuries at older ages. Cusimano et al [46] in 2011 evaluated injuries before and after the rule change. The odds of sustaining a body-checking injury increased for all age groups, except for the most novice group, which was not impacted by the rule change. Specifically, it was shown that the odds ratio (OR) for concussion was 10.08 (2.35–43.29, p=0.01) for the age group that had gone from prohibiting to allowing body-checking. The OR for all older age groups was not significant, arguing against a reduced risk of concussion for older groups when body-checking is introduced at an earlier age.
Emery and Meeuwisse[47] in 2006 demonstrated an increased risk of concussion in leagues which permit body-checking in younger age groups. Subgroup analysis based on age showed the age group for which checking is first allowed had a non-significant RR of 3.4 (0.93–18.61), but significant increases were observed for players aged 13 to 14 years old, with RR=4.04 (1.17–21.54), and those aged 15 to 16 years old, with RR=3.41 (1.02–17.87).
Emery et al [48] in 2010 examined the risk of concussion in players aged 11 to 12 years old compared between leagues that did and did not allow body-checking and found an increased incidence rate ratio (IRR) for concussion of 3.88 (1.91–7.89) when body-checking was allowed.
Emery et al [49] in 2011 evaluated whether earlier experience with body-checking impacted the risk of concussion, comparing players aged 13 to 14 years old being exposed to checking for the first time against players of the same age who carried 2 years of exposure to checking and found the risk of concussion was not significantly different: IRR=0.87 (0.51–1.50).
Hagel et al [50] evaluated risk of concussion for athletes aged 10 to 12 years old before and after the age of introduction of checking was lowered from 12 to 11. They found a significantly higher risk for concussion in athletes aged 11 years old, with RR=3.4 (1.4–8.4), but no difference in risk for players aged 10 or 12 years old.
A similar study by MacPherson et al [51] compared the risk of concussion in the 11-year-old groups in which body-checking was allowed or prohibited and also evaluated the risk among players aged 14 to 15 years old based on the extent of prior experience with body-checking. It revealed a trend toward increased risk for concussion in players aged 11 years old, with an OR=1.42 (0.98–2.05), and no difference in risk for the older group, with OR=1.6 (0.68–3.81).
Black et al [52] in 2016 demonstrated an increased risk of concussion when body-checking is allowed in youth hockey, IRR=2.83 (1.09–7.31). Black et al [53] in 2017 then compared the year before with the year after implementation of rules prohibiting body-checking in a youth hockey league and demonstrated a significant reduction in concussion risk, IRR=0.34 (0.21–0.56).
Krolikowski et al [54] found that a policy of zero tolerance for head contact did not significantly reduce the risk of concussion in youth hockey. Smith et al [55] found that Fair Play systems, which incorporate sportsmanship and penalties into youth hockey game results, did not decrease the incidence of concussion.
These results demonstrate an increased incidence of concussion associated with body-checking at younger ages and do not support the assertion that earlier introduction translates into decreased risk with increasing experience. A reduction in risk of injury would be a desirable effect of intervention. Potential undesirable effects include negative impact on the perceived quality of competition, disruption of the flow of competition caused by increasing rule infractions, and altering the culture of the game.
Recommendation: Conditional recommendation for rules governing high-risk activity as a primary preventive intervention against concussion in adult amateur athletes. Given the strength of the evidence of the association between body-checking and concussion risk, we also strongly recommend rules that prohibit body-checking at a younger age in ice hockey as an effective intervention for the primary prevention of concussion in pediatric athletes.
High-risk activity prohibition in adult amateur athletes (PICO 6)
In high school athletics 6.4% of injuries are related to prohibited activities. Of injuries caused by prohibited activity, concussion accounts for 25.4%.[56] In hockey, rule modifications have been shown to decrease overall injury rate.[57] A search of the literature revealed three studies that address rule modification and concussion.
Emery and Meeuwisse[47] compared athletes aged 15 to 16 years old for whom body-checking was allowed with those aged 9 to 10 years old for whom body-checking was prohibited, finding a significantly increased relative risk for concussion in the body-checking group, RR=3.41 (1.02–17.87). Cusimano e t al [46] in 2011 evaluated the risk of concussion based on age at which checking is introduced. For the age group 15 to 17 years old, the OR for body-checking-related concussion was not statistically significant at 1.31 (0.44–3.88), leading them to conclude that the risk of concussion at older ages was not associated with the age at which body-checking may be introduced.
A rule implemented in 2001 by the National Rugby League of Australia limited the number of player exchanges that occurred during professional play. This was associated with a lower incidence of injury, which was theorized to be due to decreased aggression in players competing in a more fatigued state.[58] Gabbett[59] investigated the incidence of concussion in amateur players after the introduction of a similar rule change. A significant decrease was demonstrated in overall risk of injury, with RR=0.70 (0.65–0.75); however, there was no difference in the risk for a composite concussion/open wound variable.As in the discussion of relevant factors for pediatric athletes, many adult amateur athletes would want rules regulating high-risk behavior as an intervention for the primary prevention of concussion, and many would not.
Recommendation: Conditional recommendation for rules governing high-risk activity as a primary preventive intervention against concussion in adult amateur athletes.
Neck mass exercises in adult amateur athletes (PICO 7)
Traumatic brain injury, including concussion, is due to linear and rotational acceleration of the head.[60] Cervical muscle contraction is theorized to more rigidly couple the head to the torso, increasing the overall mass being subjected to a force and decreasing the acceleration experienced by the brain.[61][62] This theoretical protective mechanism is the basis for exercise to increase neck mass as a preventive strategy to reduce concussion. Several studies have evaluated the relation between neck strength and acceleration in the laboratory,[63–66] but did not directly evaluate the impact on incidence of concussion. Only one study was found that evaluated the correlation between neck strength and concussion.
Collins et al [67] compared preseason neck strength measurements in 6704 high school athletes in various sports between athletes who did and did not experience concussion over two academic years. They found significantly lower neck circumference, lower neck to head circumference ratio, and lower mean overall neck strength in athletes who suffered concussions (p<0.001).No evaluation was made of the impact of neck strengthening on concussion incidence. In consideration of increasing neck strength as an intervention for the primary prevention of concussion, many adult amateur athletes would consider it an acceptable intervention.
Recommendation: Conditional recommendation for neck strengthening exercise program as a primary preventive intervention against concussion in adult amateur athletes.
Table 2 summarizes the recommendations for the seven PICO questions.

TABLE 2. EAST evidence-based recommendations for the primary prevention of contact sports-related concussions
Limitations
In the GRADE methodology, the literature is one of four factors considered in formulating recommendations.[12] Recommendations formulated in this review are primarily limited by the relative scarcity and quality of existing evidence. They serve as the rudimentary foundation for athletes, coaches, governing bodies, and injury prevention/outreach programs to formulate an evidence-based approach to concussion prevention. They also serve to augment existing guidelines addressing diagnosis and management of contact sport-related concussion. But primarily, this systematic review serves as a call for increased scientific focus on identifying and more clearly defining effective primary prevention strategies.
Conclusion
In summary, this represents the first systematic review of the literature pertaining to the primary prevention of sports-related concussion. EAST applauds the advances that have been made in the evidence guiding the diagnosis and management of mild traumatic brain injury-related to sports. However, our greatest opportunity to impact overall injury burden often lies in injury prevention. Future research will serve to more granularly define effective interventions to prevent sports-related concussion in pediatric and adult amateur athletes.
References
- PubMed search result for term “concussion”. 2017.
- Marshall S , Bayley M , McCullagh S , et al . Updated clinical practice guidelines for concussion/mild traumatic brain injury and persistent symptoms. Brain Inj 2015;29:688–700.doi:10.3109/02699052.2015.1004755
- Broglio SP , Cantu RC , Gioia GA , et al . National Athletic Trainers' Association position statement: management of sport concussion. J Athl Train 2014;49:245–65.doi:10.4085/1062-6050-49.1.07
- Harmon KG , Drezner J , Gammons M , et al . American Medical Society for Sports Medicine position statement: concussion in sport. Clin J Sport Med 2013;23:1–18.doi:10.1097/JSM.0b013e31827f5f93
- Herring SA , Cantu RC , Guskiewicz KM , et al . Concussion (mild traumatic brain injury) and the team physician: a consensus statement--2011 update. Med Sci Sports Exerc 2011;43:2412–22.doi:10.1249/MSS.0b013e3182342e64 Web of Science
- Halstead ME , Walter KD , McCambridge TM . et al . Sport-Related Concussion in Children and Adolescents. Pediatrics 2010;126:597–615.doi:10.1542/peds.2010-2005 Abstract/FREE Full Text
- McCrory P , Meeuwisse WH , Aubry M , et al . Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. J Am Coll Surg 2013;216:e55–e71.doi:10.1016/j.jamcollsurg.2013.02.020
- Emery CA , Black AM , Kolstad A , et al . What strategies can be used to effectively reduce the risk of concussion in sport? A systematic review. Br J Sports Med 2017;51:978–84.Abstract/FREE Full Text
- Guyatt GH , Oxman AD , Vist GE , et al . GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336:924–6.doi:10.1136/bmj.39489.470347.AD FREE Full Text
- Kerwin AJ , Haut ER , Burns JB , et al . The Eastern Association of the Surgery of Trauma approach to practice management guideline development using Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology. J Trauma Acute Care Surg 2012;73(5 Suppl 4):S283–S287.doi:10.1097/TA.0b013e31827013e9 PubMed
- Balshem H , Helfand M , Schünemann HJ , et al . GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 2011;64:401–6.doi:10.1016/j.jclinepi.2010.07.015 Web of Science
- Guyatt GH , Oxman AD , Kunz R , et al . Going from evidence to recommendations. BMJ 2008;336:1049–51.doi:10.1136/bmj.39493.646875.AE FREE Full Text
- ommittee on Sports Medicine and Fitness. Safety in youth ice hockey: the effects of body checking. American Academy of Pediatrics. Committee on Sports Medicine and Fitness. Pediatrics 2000;105(3 Pt 1):657–8.Abstract/FREE Full Text
- Aubry M , Cantu R , Dvorak J , et al . Summary and agreement statement of the 1st International Symposium on Concussion in Sport, Vienna 2001. Clin J Sport Med 2002;12:6–11.doi:10.1097/00042752-200201000-00005 Web of Science
- ational Center for Injury Prevention and Control. Heads Up: Concussion in High School Sports, Final Report . Atlanta, GA: Centers for Disease Control and Prevention, 2007.
- ational Center for Injury Prevention and Control. Heads Up: Concussion in Youth Sports . Atlanta, GA: Centers for Disease Control and Prevention, 2007.
- Cook DJ , Cusimano MD , Tator CH , et al . Evaluation of the ThinkFirst Canada, Smart Hockey, brain and spinal cord injury prevention video. Inj Prev 2003;9:361–6.doi:10.1136/ip.9.4.361 Abstract/FREE Full Text
- Covassin T , Elbin RJ , Sarmiento K . Educating coaches about concussion in sports: evaluation of the CDC's "Heads Up: concussion in youth sports" initiative. J Sch Health 2012;82:233–8.doi:10.1111/j.1746-1561.2012.00692.x Web of Science
- Cusimano MD , Chipman M , Donnelly P , et al . Effectiveness of an educational video on concussion knowledge in minor league hockey players: a cluster randomised controlled trial. Br J Sports Med 2014;48:141–6.doi:10.1136/bjsports-2012-091660 Abstract/FREE Full Text
- Kerr ZY , Yeargin S , Volavich McLeod TC , et al . Comprehensive coach education and practice contact restriction guidelines result in lower injury rates in youth American football. Orthop J Sports Med 2016;3:2325967116648441.
- Kerr ZY , Dalton SL , Roos KG , et al . Comparison of Indiana high school football injury rates by inclusion of the USA Football "Heads Up Football" player safety coach. Orthop J Sports Med 2016;4:2325967116648441.doi:10.1177/2325967116648441
- Gammons MR . Helmets in sport: fact and fallacy. Curr Sports Med Rep 2013;12:377–80.doi:10.1249/JSR.0000000000000016
- Thompson DC , Rivara F , Thompson R . Cochrane Injuries Group. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Syst Rev 1999;308.doi:10.1002/14651858.CD001855
- Hagel BE , Pless IB , Goulet C , et al . Effectiveness of helmets in skiers and snowboarders: case-control and case crossover study. BMJ 2005;330:281–5.doi:10.1136/bmj.38314.480035.7C Abstract/FREE Full Text
- Mueller BA , Cummings P , Rivara FP , et al . Injuries of the head, face, and neck in relation to ski helmet use. Epidemiology 2008;19:270–6.doi:10.1097/EDE.0b013e318163567c Web of Science
- Sulheim S , Holme I , Ekeland A , et al . Helmet use and risk of head injuries in alpine skiers and snowboarders. JAMA 2006;295:919–24.doi:10.1001/jama.295.8.919 Web of Science
- Bergenstal J , Davis SM , Sikora R , et al . Pediatric bicycle injury prevention and the effect of helmet use: the West Virginia experience. W V Med J 2012;108:78–81.PubMed
- McIntosh AS , McCrory P . Effectiveness of headgear in a pilot study of under 15 rugby union football. Br J Sports Med 2001;35:167–9.doi:10.1136/bjsm.35.3.167 Abstract/FREE Full Text
- McIntosh AS , McCrory P , Finch CF , et al . Does padded headgear prevent head injury in rugby union football? Med Sci Sports Exerc 2009;41:306–13.doi:10.1249/MSS.0b013e3181864bee Web of Science
- Delaney JS , Al-Kashmiri A , Drummond R , et al . The effect of protective headgear on head injuries and concussions in adolescent football (soccer) players. Br J Sports Med 2008;42:110–5.doi:10.1136/bjsm.2007.037689 Abstract/FREE Full Text
- Fukuda O , Hirashima Y , Origasa H , et al . Characteristics of helmet or knit cap use in head injury of snowboarders: analysis of 1,190 consecutive patients. Neurol Med Chir 2007;47:491–4.
- Hollis SJ , Stevenson MR , McIntosh AS , et al . Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian nonprofessional male rugby players. Am J Sports Med 2009;37:2328–33.doi:10.1177/0363546509341032 Web of Science
- Zemper ED . Cerebral concussion rates in various brands of football helmets. J Athl Train 1989;24:133–7.
- Zemper ED . Analysis of cerebral concussion frequency with the most commonly used models of football helmets. J Athl Train 1994;29:44–50.PubMed
- Pellman EJ , Viano DC , Tucker AM , et al . Committee on Mild Traumatic Brain Injury, National Football League. Concussion in professional football: location and direction of helmet impacts-Part 2. Neurosurgery 2003;53:1328–41.doi:10.1227/01.NEU.0000093499.20604.21 Web of Science
- Collins M , Lovell MR , Iverson GL , et al . Examining concussion rates and return to play in high school football players wearing newer helmet technology: a three-year prospective cohort study. Neurosurgery 2006;58:275–86.doi:10.1227/01.NEU.0000200441.92742.46 Web of Science
- Rowson S , Duma SM , Greenwald RM , et al . Can helmet design reduce the risk of concussion in football? J Neurosurg 2014;120:919–22.doi:10.3171/2014.1.JNS13916 Web of Science
- Benson BW , Mohtadi NG , Rose MS , et al . Head and neck injuries among ice hockey players wearing full face shields vs half face shields. JAMA 1999;282:2328–32.doi:10.1001/jama.282.24.2328 Web of Science
- Benson BW , Rose MS , Meeuwisse WH . The impact of face shield use on concussions in ice hockey: a multivariate analysis. Br J Sports Med 2002;36:27–32.doi:10.1136/bjsm.36.1.27 Abstract/FREE Full Text
- Stuart MJ , Smith AM , Malo-Ortiguera SA , et al . A comparison of facial protection and the incidence of head, neck and facial injuries in junior A hockey players. Am J Sports Med 2002;30:39–44.doi:10.1177/03635465020300012001 PubMedWeb of Science
- Marshall SW , Loomis DP , Waller AE . Evaluation of protective equipment for prevention of injuries in rugby union. Int J Epidemiol 2005;34:113–8.doi:10.1093/ije/dyh346 Web of Science
- McGuine TA , Hetzel S , McCrea M , et al . Protective equipment and player characteristics associated with the incidence of sport-related concussion in high school football players: a multifactorial prospective study. Am J Sports Med 2014;42:2470–8.doi:10.1177/0363546514541926 Web of Science
- Collins CL , McKenzie LB , Ferketich AK , et al . Concussion characteristics in high school football by helmet age/recondition status, manufacturer, and model. Am J Sports Med 2016;44:1382–90.doi:10.1177/0363546516629626
- Greenhill DA , Navo P , Zhao H , et al . Inadequate helmet fit increases concussion severity in American high school football players. Sports Health 2016;8:238–43.doi:10.1177/1941738116639027
- Marar M , McIlvain NM , Fields SK , et al . Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med 2012;40:747–55.doi:10.1177/0363546511435626 Web of Science
- Cusimano MD , Taback NA , McFaull SR , et al . Canadian Research Team in Traumatic Brain Injury and Violence. Effect of bodychecking on rate of injuries among minor hockey players. Open Med 2011;5:e57–64.PubMed
- Emery CA , Meeuwisse WH . Injury rates, risk factors, and mechanisms of injury in minor hockey. Am J Sports Med 2006;34:1960–9.doi:10.1177/0363546506290061 Web of Science
- Emery CA , Kang J , Shrier I , et al . Risk of injury associated with body checking among youth ice hockey players. JAMA 2010;303:2265–72.doi:10.1001/jama.2010.755 Web of Science
- Emery C , Kang J , Shrier I , et al . Risk of injury associated with bodychecking experience among youth hockey players. CMAJ 2011;183:1249–56.doi:10.1503/cmaj.101540 Abstract/FREE Full Text
- Hagel BE , Marko J , Dryden D , et al . Effect of bodychecking on injury rates among minor ice hockey players. CMAJ 2006;175:155–60.doi:10.1503/cmaj.051531 Abstract/FREE Full Text
- Macpherson A , Rothman L , Howard A . Body-checking rules and childhood injuries in ice hockey. Pediatrics 2006;117:e143–e147.doi:10.1542/peds.2005-1163 Abstract/FREE Full Text
- Black AM , Macpherson AK , Hagel BE , et al . Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med 2016;50:55–61.doi:10.1136/bjsports-2015-095103 Abstract/FREE Full Text
- Black A , Palacios-Derflingher L , Schneider KJ , et al . The effect of a national body checking policy change on concussion risk in youth ice hockey players. Br J Sports Med 2017;51:A70.3–A71.doi:10.1136/bjsports-2016-097270.183
- Krolikowski MP , Black AM , Palacios-Derflingher L , et al . The effect of the “zero tolerance for head contact” rule change on the risk of concussions in youth ice hockey players. Am J Sports Med 2017;45:468–73.doi:10.1177/0363546516669701
- Smith AM , Gaz DV , Larson D , et al . Does fair play reduce concussions? A prospective, comparative analysis of competitive youth hockey tournaments. BMJ Open Sport Exerc Med 2016;2:e000074.doi:10.1136/bmjsem-2015-000074
- Collins CL , Fields SK , Comstock RD . When the rules of the game are broken: what proportion of high school sports-related injuries are related to illegal activity? Inj Prev 2008;14:34–8.doi:10.1136/ip.2007.017277 Abstract/FREE Full Text
- Roberts WO , Brust JD , Leonard B , et al . Fair-play rules and injury reduction in ice hockey. Arch Pediatr Adolesc Med 1996;150:140–5.doi:10.1001/archpedi.1996.02170270022003 Web of Science
- Orchard J , Steet L , Walker C . Effect of limited interchange rule on players leaving the field at an NRL club : Sportslink, 2003:12–14.
- Gabbett TJ . Influence of the limited interchange rule on injury rates in sub-elite Rugby League players. J Sci Med Sport 2005;8:111–5.doi:10.1016/S1440-2440(05)80031-3
- Grossman RG , Gildenberg PL Gennarelli TA , Seggawa H , Wald U . Physiological response to angular acceleration of the head. In: Grossman RG , Gildenberg PL , Head Injury: Basic and Clinical Aspects . New York, NY: Raven Press, 1982:129–40.
- Simoneau M , Denninger M , Hain TC . Role of loading on head stability and effective neck stiffness and viscosity. J Biomech 2008;41:2097–103.doi:10.1016/j.jbiomech.2008.05.002 Web of Science
- Viano DC , Casson IR , Pellman EJ . Concussion in professional football: biomechanics of the struck player--part 14. Neurosurgery 2007;61:313–27.doi:10.1227/01.NEU.0000279969.02685.D0 Web of Science
- Tierney RT , Sitler MR , Swanik CB , et al . Gender differences in head-neck segment dynamic stabilization during head acceleration. Med Sci Sports Exerc 2005;37:272–9.doi:10.1249/01.MSS.0000152734.47516.AA Web of Science
- Mansell J , Tierney RT , Sitler MR , et al . Resistance training and head-neck segment dynamic stabilization in male and female collegiate soccer players. J Athl Train 2005;40:310–9.PubMedWeb of Science
- Mihalik JP , Guskiewicz KM , Marshall SW , et al . Does cervical muscle strength in youth ice hockey players affect head impact biomechanics? Clin J Sport Med 2011;21:416–21.doi:10.1097/JSM.0B013E31822C8A5C
- Schmidt JD , Guskiewicz KM , Blackburn JT , et al . The influence of cervical muscle characteristics on head impact biomechanics in football. Am J Sports Med 2014;42:2056–66.doi:10.1177/0363546514536685
- Collins CL , Fletcher EN , Fields SK , et al . Neck strength: a protective factor reducing risk for concussion in high school sports. J Prim Prev 2014;35:309–19.doi:10.1007/s10935-014-0355-2