Prevention Firearm Injuries with Gun Safety Devices and Safe Storage (UPDATE IN PROGRESS)
Published 2018
Citation: J Trauma. 84(6):1003-1011, June 2018
Authors
Violano, Pina, PhD; Bonne, Stephanie, MD; Duncan, Thomas, DO; Pappas, Peter, MD; Christmas, A., Britton, MD; Dennis, Andrew, DO; Goldberg, Stephanie, MD; Greene, Wendy, MD; Hirsh, Michael, MD; Shillinglaw, William, DO; Robinson, Bryce, MD; Crandall, Marie, MD
Author Information
From the Injury Prevention Center, Yale-New Haven Hospital (P.V.), New Haven, Connecticut; Division of Trauma/Surgical Critical Care, Rutgers New Jersey Medical School (S.B.), Newark, New Jersey; Department of Trauma Services, Ventura County Medical Center (T.D.), Ventura, California; Department of Surgery, University of Central Florida College of Medicine (P.P.), Orlando, Florida; Department of Surgery, Carolinas Health Care (A.B.C), Charlotte, North Carolina; Department of Trauma, Cook County Hospital (A.D.), Chicago, Illinois; Division of Acute Care Surgical Services, Virginia Commonwealth University (S.G.), Richmond, Virginia; Acute and Critical Care Surgery, Emory University School of Medicine (W.G.), Atlanta, Georgia; Pediatric Surgery and Trauma, University of Massachusetts (M.H.), Boston, Massachusetts; Mission Trauma Services, Mission Hospitals Asheville (W.S.), Asheville, North Carolina; and Trauma, Burn, & Critical Care, University of Washington Harborview Medical Center (B.R.), Seattle, Washington.
Submitted: January 22, 2018, Revised: February 27, 2018, Accepted: March 1, 2018, Published online: March 8, 2018.
Address for reprints: Marie Crandall, MD, University of Florida College of Medicine Jacksonville, 655 W. 8th Street, Jacksonville, FL 32209; email: [email protected].
Abstract
BACKGROUND Over 50,000 homicides and suicides occur each year. An estimated half of all US households are believed to have a firearm present, making them one of the most ubiquitous consumer products. Our goal was to determine if the manner of storage of a firearm in a home could potentially make a difference in the outcomes of intentional and unintentional injuries involving a firearm; specifically addressing the use of gun safes and devices that block/disable firearm function (trigger locks, cable locks, etc.).
METHODS A comprehensive review of the literature was performed. We used Grading of Recommendations Assessment, Development, and Evaluation methodology to assess the breadth and quality of the data specific to our Population, Intervention, Comparator, Outcomes (PICO) questions.
RESULTS A total of 176 studies were initially identified, then, 120 more added after a subsequent literature review, with 97 removed as duplicates. One hundred ninety-one case reports, case series, and reviews were removed because they did not focus on prevention or did not address our comparators of interest. This left a total of two studies which merited inclusion for PICO 1, should gun locks be used to prevent firearm injuries and six studies which merited inclusion for PICO 2, should safe storage for guns be used to prevent firearm injuries.
CONCLUSION PICO 1: We conditionally recommend that gun locks be used to prevent unintentional firearm injury. PICO 2: Because of the large effect size and the reasonable quality of available evidence with safe storage of firearms, we recommend safe storage prevent firearm-related injuries.
LEVEL OF EVIDENCE Systematic review, level III.
Overview
Over 50,000 homicides and suicides occur each year in the United States.[1] In 2015, homicide was the second leading cause of death, and suicide the third for persons 15 years to 24 years of age.[2] Approximately 60% of all homicides and suicides in the United States are committed with a firearm. Although unintentional firearm-related injuries are less likely to result in death, those who survive gunshot wounds can be subject to long-term sequelae associated with physical impairment and permanent disability.[3]
The presence of a household firearm is associated with an increased risk of suicide among adults and adolescents.[4]Adolescent suicide completers were 2.5 times more likely to have a gun in their home than were diagnostically similar, psychiatrically ill, suicidal children, thus suggesting that the availability of firearms represents a significant risk factor for suicide.[5] Other work suggests that the presence of a gun in the home is much more likely to result in a suicide than in a defensible homicide.[5] Firearms were the cause of nearly 51% of US suicide deaths from 2004 to 2012, never falling below 50% in any year.[6][7]
In the United States, there are over 200 million firearms in civilian hands, far more than in any other developed nation. There are also far more firearm related injuries.[8] Hand-guns are present in more than half of US households with firearms, about one in five households overall.[8] A recent practice management guideline generated by the Eastern Association for the Surgery of Trauma (EAST) Injury Control and Violence Prevention Section concluded that more restrictive licensing gun laws is associated with lower firearm injuries,[9] but given the volatile debate about second amendment rights versus public health, universal restrictive licensing is unlikely.
Unloading and locking all guns and ammunition in the home can potentially reduce access to guns by youth. Securely storing guns is perhaps a more plausible strategy for intentional gun injuries among toddlers and young children, but its effectiveness to reduce youth suicide is less clear.
The purpose of this systematic review was to determine if the manner of storage of a firearm in a home could make a difference in firearm injuries; specifically addressing storage of a loaded or unloaded firearm in a secure vs unsecure location, and evaluating outcomes of devices that block/disable firearm function (trigger locks, cable locks, etc).
Objectives
The objective of this systematic review was to evaluate the use of firearm storage devices and safety devices that block/disable the firing function of a firearm (trigger locks, cable locks, etc) to prevent intentional and unintentional firearm-related injuries.
A broad-based committee of surgeons and nurses was formed from the membership of the EAST Injury Control and Violence Prevention Section, and the EAST Guidelines Committee. The team included individuals with a range of research experience and many with military and/or civilian law enforcement backgrounds. We created the Populations, Intervention, Comparator, and Outcome (PICO) questions of interest and created a list of potential outcomes. The group voted any type of firearm injury, fatal or nonfatal, irrespective of intent, as critically important. No external funding was used for this project.
PICO Questions
For this review, two PICO questions were estimated by the authors as the most salient aspects of injury related to firearm safety practices.
PICO Question 1, firearm safety devices
- Patient population: general population
- Intervention: firearm safety devices that block/disable the firing function (trigger locks, cable locks, etc)
- Comparators: with and without firearm safety devices
- Outcome: all firearm injuries
PICO 2, safe firearm storage
- Patient population: general population
- Intervention: gun storage
- Comparators: with and without gun storage
- Outcome: all firearm injuries
Materials and Methods
Inclusion Criteria for this Review
Study Types
Studies included randomized controlled trials, prospective and retrospective observational studies, ecological studies, and case-control studies. Case reports, conceptual pieces, and reviews containing no original data or analyses were excluded. We excluded editorials, opinion articles, and studies not addressing the PICO questions. We included all studies published between January 1, 1900, and June 30, 2017. We did not restrict by publication language or limit our analysis to studies of the United States population.
Participant Types
We included all relevant studies, irrespective of age, race, sex, or other demographic characteristics.
Intervention Types
We reviewed all studies which evaluated the effects of firearm storage devices and firearm safety devices on the prevention of firearm-related injuries.
Outcome Measure Types
We limited the review to studies in which an injury as a result of a firearm was the outcome; we included fatal and nonfatal injuries, and included both intentional and unintentional mechanisms.
Review Methods
Search Strategy
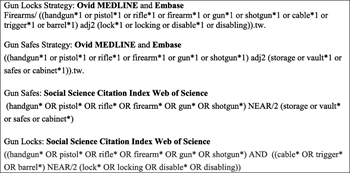
FIGURE 1. Search strategy 1—Yale librarian
In January 2017, an institutional research librarian performed a systematic search of Ovid, MEDLINE, Embase, and Social Sciences Citation Index (Web of Science). The search strategies were devised to favor precision over recall. Figure 1 contains the MeSH terms used for the initial search.

FIGURE 2. Search strategy 2—Florida librarian
In keeping consistent with previous systematic reviews, a second search was completed to include additional social science databases: Cochrane Central Register of Controlled Trials, Web of Science Core Collection PsychINFO, CINAHL, Art and Humanities Citation Index, and Conference Proceedings Citation Index. A second institutional research librarian performed this literature search which found 120 additional relevant articles (Fig. 2).
Study Selection
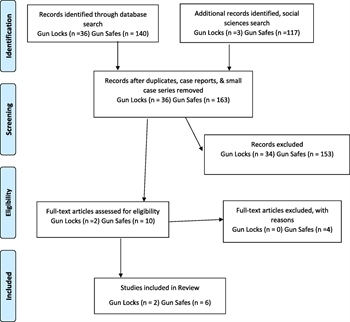
FIGURE 3. PRISMA Flow Diagram
Two independent reviewers (P.V., M.C.) then screened titles and abstracts, excluding reviews, case reports, and unrelated articles. The resulting studies were used for the review. The study selection process is highlighted in the PRISMA flow diagram for Figure 3.
A total of 39 abstracts were identified in our initial searches for PICO 1 and 257 abstracts for PICO 2. Duplicates, case reports, and small-case series were excluded (n = 3) for PICO 1 and (n = 94) for PICO 2. The authors then reviewed the articles for relevance and excluded articles that did not include injury as a specific outcome of interest (n = 34 for PICO 1; n = 153 for PICO 2). Articles not relevant to our specific PICO questions (n = 0 for PICO 1; n = 4 for PICO 2) were also excluded.
There were no additional articles added to the literature summary after reading relevant review articles (n = 0). The final list of two articles for PICO 1 and six for PICO 2 were reviewed and used to create the recommendations. Finally, a focused search update in October 2017 demonstrated no new relevant articles.
Data Extraction and Management
All references used for the review were entered into a Microsoft Excel (Microsoft Corporation, Redmond, WA) spreadsheet containing information on authors, article title, study methodology, and intervention and outcome measures. A master copy was made available to all reviewers. All articles, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) resources, and instructions were electronically available to all members of the writing team. Each independent reviewer shared his or her PICO sheet and literature review with all members of the team. Independent interpretations of the data were shared through group email and conference calls. There were a few reviewer discrepancies in grading that occurred. A modified Delphi technique was used to resolve differences. Grading was completed in July 2017.
Methodological Quality Assessment
We used the validated GRADE methodology for this study.[10–12] The GRADE methodology entails the creation of a predetermined PICO question or set of PICO questions that the literature aims to answer. Each designated reviewer independently evaluates the data in aggregate with respect to the quality of the evidence to adequately answer each PICO question and quantified the strength of any recommendations. Reviewers are asked to determine effect size, risk of bias, inconsistency, indirectness, precision, and publication bias.
Recommendations are based on the overall quality of the evidence on the participant. GRADE methodology suggests the phrases, “we recommend” for strong evidence, and “we conditionally recommend” for weaker evidence.
Outcome Measure Types
We limited the review to studies in which injury was the outcome, not simply firearm storage devices or disabling devices. Owing to the heterogeneity of injury reports, all injuries including, but not limited to, gunshot wounds were felt to be essential to evaluating the literature within the GRADE framework.
Results
Two articles met inclusion criteria for PICO 1 and six articles for PICO 2. All studies were primarily written in English and from United States institutions.
Results: Should Firearm Safety Devices be Used to Prevent Firearm Injuries? (PICO 1)

TABLE 1. PICO 1
Two studies were available for review for PICO 1 (Table 1). In 1996, Sinauer et al.[3] performed an observational study of firearm injuries in which they extracted firearm related injury cases from the National Electronic Injury Surveillance System data set from June 1, 1992 through May 31, 1994. National Electronic Injury Surveillance System is a stratified sampling dataset that, at the time, comprised 91 hospitals emergency departments, intended to represent a probability sample of all hospitals in the United States. Using the data from this sample, the study estimated an unintentional firearm injury rate of 6.7/100,000 during this period. The injuries occurred in men 87% of the time, 70% were self-inflicted, and 73% involved an extremity. In 70% of the cases, the activity associated with the unintentional injury was identified, most often, this was gun cleaning (14%), hunting (12%), or handling (31%). Handling-related injuries occurred when individuals were showing the gun to others, carrying the gun, looking at a gun, or playing with the gun. The study provided indirect evidence that firearm safety devices might decrease injuries in those circumstances. The study is limited because it only indirectly addressed gun safety practices and was not generalizable to intentional injury.
Grossman et al.[4] examined the role of unsecured weapons in unintentional pediatric firearm injuries. Firearms involved in an incident in which a child or adolescent less than 20 years accidentally shot another individual of any age were identified from hospital or medical examiners reports. These weapons were matched using case-control methodology to weapons identified by random-digit dialing. Interviews of the weapons' owners and others in the household then identified the storage practices of the firearm in question. A total of 106 respondents were interviewed, with 480 control firearms. The study found lower risk of injury or death in firearms stored unloaded (odds ratio [OR], 0.30; 95% confidence interval [CI], 0.16–0.56), locked (OR, 0.27; 95% CI, 0.17–0.45), separately from ammunition (OR, 0.45; 95% CI, 0.34–0.93), and where ammunition was locked (OR, 0.39; 95% CI, 0.23–0.66). Limitations of the study included sampling and recall bias, it being a selected study rather than population-based, and generalizability, given that most cases were from the Pacific Northwest.
In grading the above studies with respect to PICO 1, reviewers noted significant risk of bias, inconsistency, imprecision, and indirectness in the conclusions from these studies. However, there was really no plausible confounding that would change the effect noted in the two studies. Despite concerns for the small studies and low amount of data, reviewers noted the large magnitude of the effect; therefore, we conditionally recommend that firearm safety devices, such as gun locks, be used to prevent unintentional firearm injury.
Results: Should Safe Storage for Guns be Used to Prevent Firearm Injuries? (PICO 2)
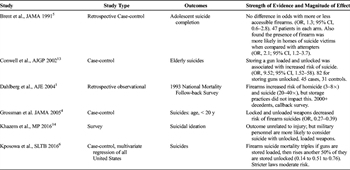
TABLE 2. PICO 2
Six articles were reviewed for PICO 2, four case-control studies, one retrospective observational study, and one survey (Table 2). In 1991, Brent et al.[5] performed a case-control study of 47 adolescent suicide victims. A control group of psychiatric in-patients who had attempted suicide and a second control group of never-suicidal psychiatric inpatients were matched to the victims on age, sex, and geography. The odds of a presence of a gun in the home of a suicide victim was calculated. This study found that guns were twice as likely to be found in the home of adolescents who completed suicides (OR, 2.2; 95% CI, 1.4–3.5) when compared with controls. There was no evidence that the method of storage of the firearm lessened the risk of suicide, simply the presence or absence of the firearm in the home was related to the risk. The study is limited by the retrospective nature of the review and recall bias on the part of the participants and controls.
In 2002, Conwell et al.[13] performed a similar case-control study evaluating elderly (50 years and older) suicide victims and a matched cohort of individuals of the same age, sex, living situation, and education level from the same geographic area. Post hoc matching also accounted for Axis 1 psychiatric diagnoses. The study evaluated 45 suicides by firearm and 31 controls. The presence of any firearm in the home was found to be an increased risk factor for suicide in men (OR, 3.17; 95% CI, 1.83–11.22), as did the presence of a handgun in the home (OR, 2.57; 95% CI, 1.71–13.11). Having only a long gun in the home did not increase suicide risk and presence of any firearm did not increase suicide risk among women. Storage of the firearm, however, was an independent predictor of suicide risk, both by storing the weapon loaded (OR, 9.52; 95% CI, 1.52–58.82) or unlocked (OR, 6.41; 95% CI, 1.17–35.71). Limitations of the study included not controlling for psychiatric disease, participation bias (many contacted families did not participate), and the small study population from a geographically limited area.
The Grossman et al.[4] study described for PICO 1 was also evaluated for PICO 2. In this context, the authors noted that storing household guns as locked, unloaded, or separate from the ammunition was associated with significant reductions in the risk of unintentional injury and self-inflicted firearm injuries and deaths among children and adolescents. Again, this study found lower risk of injury or death in firearms stored unloaded (OR, 0.30; 95% CI, 0.16–0.56), locked (OR, 0.27; 95% CI, 0.17–0.45), separately from ammunition (OR, 0.45; 95% CI, 0.34–0.93) and where ammunition was locked (OR, 0.39; 95% CI, 0.23–0.66).
The final, most recent case-control study we evaluated was performed by Kposowa et al.[6] in 2016. This study examined both the storage practices and the state firearm regulations on state-level suicide rates and applied a multivariate analysis to the most recent available mortality and census data available for 49 of the 50 states in the United States. Mixed models were used to compile data from the Centers from Disease Control and Prevention (CDC), the Law Center to Prevent Gun Violence and the United States Bureau of the Census to create an overall model of firearm regulatory practices in each state, including past survey data from those states regarding firearm storage methods. States were matched on demographic measures, such as long-term unemployment and divorce rates, and then compared across nine census divisions. Suicide rates were higher in states with higher levels of gun ownership. In this study, the risk of firearm suicide mortality triples if guns are stored loaded and also rises by 50% if the gun is stored unlocked, demonstrating a strong association of storage practices on suicide rates. This study was limited by the time frame of data collection of household level firearm data, which was collected in 2004 and 2005 and compared with suicide rates from 2011, 2012, and 2013. These data can also not currently be replicated because state-level survey data regarding firearm ownership has been absent from the CDC’s Behavioral Risk Factor Surveillance System surveys since 2005, and state-level firearm ownership data is incomplete due to state and federal regulations limiting such data collection and record keeping.
In 2004, Dahlberg et al.[1] evaluated data from the National Mortality Follow-back Survey. This survey was sent by the CDC to a sample of decedents aged 15 years and older in the United States. Survey data from 1993 were used for this study. Death certificate data and proxy interviews were collected, with a wide range of interview topics including access to health care, life events, daily activities, and a number of questions about firearms in the home of the decedent. Decedents were divided into three groups—suicide, homicide, or other, and compared by measures of firearm availability. Nearly 75% of decedents of suicide lived in a home with a firearm, compared with 42% of homicide victims and 33% of those who died of other causes. The adjusted odds ratio, based on demographic and other factors, for death by homicide in a home with a firearm was 1.9 (95% CI, 1.1–3.4), and for suicide was 10.4 for males (95% CI, 5.8–18.9) and 2.3 for women (95% CI, 1.0–5.0). The authors concluded that there was a strong higher risk for dying a violent death for those who live in a home with a firearm, and that risk increases if the firearm is unlocked or loaded. The limitations of this study include that it was retrospective and relied on proxy interviews and was limited to deaths that occurred in the home, and there is no evidence that the gun in the home was the one that was involved in the death.
A single-survey study was reviewed from Khazem et al.[14] This study surveyed 432 active duty military personnel who endorsed current firearm ownership from a military base in the southern United States. Participants were asked about their firearm storage techniques and then assessed for suicidal ideation and for self-reported past suicide attempts and likelihood of a future suicide attempt. The study found that firearm storage moderated the relationship between suicidal ideation and suicide attempts such that the likelihood of a future suicide attempt was greater in those individuals who stored their guns unlocked and loaded. The authors concluded that this supports the findings of other studies that indicate an increased risk of suicide in homes in which a gun is stored unlocked and loaded. This study is limited by small sample size in a geographically constricted military population and by self-reported survey methods and outcomes.
For PICO 2, the reviewers noted that the quality of the evidence is somewhat low, although not as low as with PICO 1. There was noted to be some risk of bias, but no inconsistency, no indirectness, no imprecision and low likelihood of publication bias. The dose-response gradient was found to be present, as well as a very large effect without plausible confounding. Because of the large effect size and the reasonable quality of available evidence with safe storage, we recommend safe storage to prevent firearm injuries.
Discussion
Firearm injury is a significant cause of injury in the United States, with thousands of unintentional firearm injuries and suicides annually. Methods to prevent firearm injury remain controversial, owing to concerns that restrictive access and storage regulations violate the constitutional right to bear arms afforded by the second amendment. Physicians and public health practitioners should continue to evaluate the available evidence and recommend safe storage and handling of the weapon as a means of protection from unintentional injury, suicide, or homicide.[15][16] Though we know that programs to improve safe firearm storage can influence behaviors,[16–18] our goal was to determine the effects on firearm injury prevention.
In studying firearm safety, several challenges were noted. The overall quality of evidence was weak; there were no randomized controlled clinical trials, and there was a paucity of evidence particularly for the question of gun locks. Finally, many sources of bias were found, including recall bias and publication bias that might have affected our results. However, despite significant limitations in study design and data quality in individual studies, the studies all came to similar conclusions and the magnitude of the effect was great enough for us to make recommendations.
Recommendations

FIGURE 4. Summary of recommendations
Should firearm safety devices be used to prevent firearm injuries? (PICO 1)
Recommendation: We conditionally recommend the use of firearm safety devices to decrease the incidence of unintentional firearm injuries ( Figure 4 ).
Despite the paucity of quality evidence to support gun locks, the magnitude and importance of effect is large, leading to the conditional recommendation for the use of gun locks by this review. It has been demonstrated that access to a firearm is a risk for completion of suicide attempts among adolescents.[19][20] It has also been demonstrated that the distribution and teaching of gun lock use can increase safe storage practices.[21]The theoretical benefit of restricting firearm access to children and adolescents, as well as lethal means access to those who are suicidal is high. Many communities, acting on this theory, have initiated free gun lock programs and education for families such as Project ChildSafe.[22] The Veterans Administration has followed with free gun locks for veterans,[23] citing that the time it takes to remove the gun lock may be enough for the individual to reconsider their suicidal ideations. These concepts are not well supported by the literature but nonetheless are worthy of further study considering the low cost and easy distribution of these devices weighed against the extent of possible effect for public health and society.
Should safe storage for guns be used to prevent firearm injuries? (PICO 2)
Recommendation: We recommend the use of safe storage of firearms as a means of prevention of firearm injury ( Figure 4 ).
A number of studies used in this review postulate that access to firearms increases the risk of both homicide and suicide. Recommendations from the American Academy of Pediatrics, the National Shooting Sports Foundation and numerous other major organizations suggest that firearms should be stored locked, unloaded, and separate from ammunition. In the case of a suicidal or homicidal individual, easy and quick access to a loaded weapon is demonstrated in all studies we reviewed to increase the risk of completing the intended suicide or homicide.[1][4–6][13][14] Owning a firearm and the presence of a firearm in the home with suicidal adolescents or middle aged adults have been shown to increase the risk of a completed suicide.[19][24][25] Additional studies on the epidemiology of suicide have noted that when less lethal means are used (attempted lethal overdose, hanging) and survived, the individual makes a second suicide attempt in only 10% of cases.[26] This suggests that a large percentage of individuals who commit suicide by firearm are prey to impulsivity plus lethality of means. These individuals, presumably, would receive appropriate treatment and not make a second suicide attempt. Similarly, the population-level rate of suicide by firearm is higher in states or regions that have higher firearm ownership rates.[27]
The quality of the evidence in this review is limited, specifically by the retrospective nature of these studies, the interview nature of the data collection which may be subject to recall bias, and some small sample sizes. However, all studies conclude that safe storage of firearms decrease the risk of suicide, with one study also stating it decreases the risk of homicide in the home. Given the magnitude of the effect, we conclude that safe storage should receive a strong recommendation to prevent firearm injury, in particular from suicide and homicide in the home setting.
Using These Guidelines in Clinical Practice
Many trauma centers see gun violence as a significant percentage of their overall trauma burden. As part of the injury prevention mission of the trauma community, trauma centers should consider the dissemination of information and potentially free supplies to encourage safe storage and locking of guns in their community. Ideally, this should be part of a multidisciplinary approach to gun injury prevention in coordination with community partners and other trauma system stakeholders. Finally, as part of their responsibilities to injured patients and their communities, trauma care providers should continue to advocate for robust research and funding for research to study these and other strategies for prevention of firearm related injuries.
Conclusion
After review of the available evidence regarding gun locks and safe storage, we found a limited association between gun locks and a moderate association between safe storage and decreased firearm injury. Further updates and additional study will continue to inform the trauma community and lay public about the potential advantages of gun locks and safe storage of firearms.
Authorship
M.C., P.V., T.D. designed this study. P.V. and M.C. conducted the literature search. P.V., S.B., T.D., P.P., A.B.C., A.D., S.G., W.G., M.H., W.S., B.R., and M.C. graded the evidence. M.C., S.B., B.R., and P.V. interpreted the data. M.C., P.V., S.B., P.P. and T.D. prepared the manuscript. P.V. and M.C. edited the manuscript.
Disclosure
The authors declare no conflicts of interest.
References
- Dahlberg LL, Ikeda RM, Kresnow M. Guns in the home and risk of a violent death in the home: findings from a national study. Am J Epidemiol. 2004;160(10):929–936.
- Centers for Disease Control and Prevention. (2017, May 2). 10 leading causes of injury deaths by age group highlighting unintentional injury deaths, United States—2015. Accessed on November 18, 2017 from http://www.cdc.gov/injury/wisqars/pdf/10LCID_Unintentional_Deaths_2015-a.pdf.
- Sinauer N, Annest JL, Mercy JA. Unintentional, nonfatal firearm-related injuries. A preventable public health burden. JAMA. 1996;275(22):1740–1743.
- Grossman DC, Mueller BA, Riedy C, Dowd MD, Villaveces A, Prodzinski J, Nakagawara J, Howard J, Thiersch N, Harruff R. Gun storage practices and risk of youth suicide and unintentional firearm injuries. JAMA. 2005;293(6):707–714.
- Brent D, Perper J, Allman C, Moritz G, Wartella M, Zelenak J. The presence and accessibility of firearms in the homes of adolescent suicides—a case-control study. JAMA. 1991;266(21):2989–2995.
- Kposowa A, Hamilton D, Wang K. Impact of firearm availability and gun regulation on state suicide rates. Suicide Life-Threat Behav. 2016;46(6):678–696.
- Center for Disease Control. 2015. WISQARS fatal injury reports. Retrieved October 17, 2017 from https://webappa.cdc.gov/sasweb/ncipc/mortrate.html.
- Miller M. One third of households in the USA own firearms which are often stored unsafely. Evid Base Healthc Publ Health. 2005;9(1):23–25.
- Crandall M, Eastman A, Violano P, Greene W, Allen S, Block E, Christmas AB, Dennis A, Duncan T, Foster S, et al. Prevention of firearm-related injuries with restrictive licensing and concealed carry laws: an Eastern Association for the Surgery of Trauma Systematic Review. J Trauma Acute Care Surg. 2016;81(5):952–960.
- Jaeschke R, Guyatt GH, Dellinger P, Schünemann H, Levy MM, Kunz R, Norris S, Bion J. GRADE Working Group. Use of GRADE grid to reach decisions on clinical practice guidelines when consensus is elusive. BMJ. 2008;337:a744.
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schunemann HJ. GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926.
- Kerwin AJ, Haut ER, Burns JB, Como JJ, Haider A, Stassen N, Dahm P. Eastern Association for the Surgery of Trauma Practice Management Guidelines Ad Hoc Committee. The Eastern Association of the Surgery of Trauma approach to practice management guideline development using Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S283–S287.
- Conwell Y, Duberstein PR, Connor K, Eberly S, Cox C, Caine ED. Access to firearms and risk for suicide in middle-aged and older adults. Am J Geriatr Psychiatry. 2002;10(4):407–416.
- Khazem LR, Houtsma C, Gratz KL, Tull MT, Green BA, Anestis MD. Firearms matter: the moderating role of firearm storage in the association between current suicidal ideation and likelihood of future suicide attempts among united states military personnel. Mil Psychol. 2016;28(1):25–33.
- Morrissey TW. Associations between active shooter incidents and gun ownership and storage among families with young children in the United States. Prev Med. 2017;100:50–55.
- Runyan C, Brooks-Russell A, Betz M, Brandspigel S, Tung G, Novins D, Agans R. Law enforcement agencies’ and gun retailers’ roles in gun storage for suicide prevention. Inj Prev. 2017;23:A47.
- U.S. Government Accountability Office. Personal Firearms: Programs that Promote Safe Storage and Research on their Effectiveness. GAO-17-665. September 19, 2017. Accessed at http://www.gao.gov/mobile/products/GAO-17-665?utm_medium=social&utm_source=twitter&utm_campaign=usgao.
- Jenco M. Study: 39% of Parent Wrongly Believe Children Don’t Know Where Gun is Stored. May 23, 2017. American Academy of Pediatrics News. Accessed on October 30, 2017 at http://www.aappublications.org/news/2017/05/23/Firearms052317.
- Brent DA, Perper JA, Moritz G, Baugher M, Schweers J, Roth C. Firearms and adolescent suicide. A community case-control study. Am J Dis Child. 1993;147:1066–1071.
- Brent D, Bridge J. Firearms availability and suicide: evidence, intervention, and future directions. Am Behav Sci. 2003;46(9):1192–1210.
- Carbone PS, Clemens CJ, Ball TM. Effectiveness of gun-safety counseling and a gun lock giveaway in a Hispanic community. Arch Pediatr Adolesc Med. 2005;159(11):1049–1054.
- Project ChildSafe 2017. www.projectchildsafe.org[website; accessed November 2017].
- U.S. Department of Veterans Affairs. “One question can make a difference”. https://spreadtheword.veteranscrisisline.net/wp-content/uploads/2014/06/email-newsletter-mar-2016.pdf[website,.pdf; accessed November 2017].
- Siegel M, Rothman EF. Firearm ownership and suicide rates among US men and women, 1981–2013. Am J Public Health. 2016;106(7):1316–1322.
- Berman AL, Brent DA, Christoffel KK. Youth Suicide by Firearms Task Force. Consensus statement on youth suicide by firearms. Arch Suicide Res. 1998;4(1):89–94.
- van Aalst JA, Shotts SD, Vitsky JL, Bass SM, Miller RS, Meador KG, Morris JA. Long-term follow-up of unsuccessful violent suicide attempts: risk factors for subsequent attempts. J Trauma. 1992;33(3):457–464.
- Miller M, Hemenway D, Azrael D. Firearms and suicide in the northeast. J Trauma. 2004;57(3):626–632.
Keywords:
Evidence-based review; systematic review; firearm injury; injury prevention